
The 1 in 31 Debate: Why Autism Numbers are Rising and Why Data Matters More Than Headlines
*Written under the supervision of Register Behaviour Analysts (RBAs), Renee Hacker, Clinical Director at Lake Ridge Community Support Services.
Recently, the autism spectrum has come under intense scrutiny. As prevalence rates climb—with some data now suggesting that up to 1 in 31 people are autistic—a divide has emerged. On one side are those who see the evolution of diagnostic criteria; on the other are those who find the volume of new diagnoses "crazy" or concerning.
At LRCSS, we have been on this journey for 40 years. We have seen the shift from the back wards of institutions to the vibrant, neurodiverse communities of today. As Behaviour Analysts and clinicians, we prefer to ground our decisions in data, not headlines.
To understand where we are going, we have to look at the science of how we got here.
The Evolution of the "1 in 31"
It is easy to look at a graph and see a "spike," but a spike in data usually indicates that we’ve started looking in the right places.
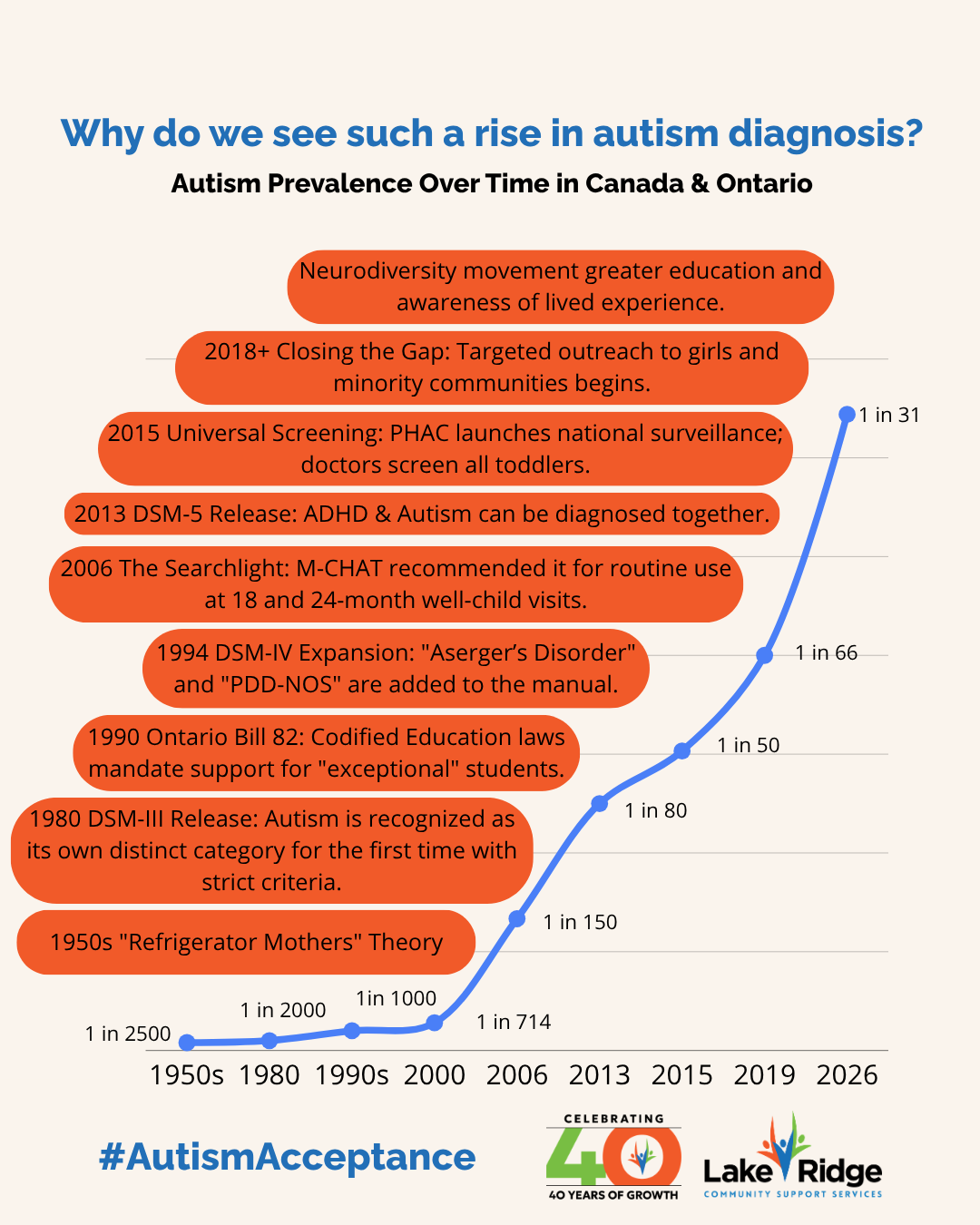
1. The Era of "Infantile Autism" (1940s–1970s)
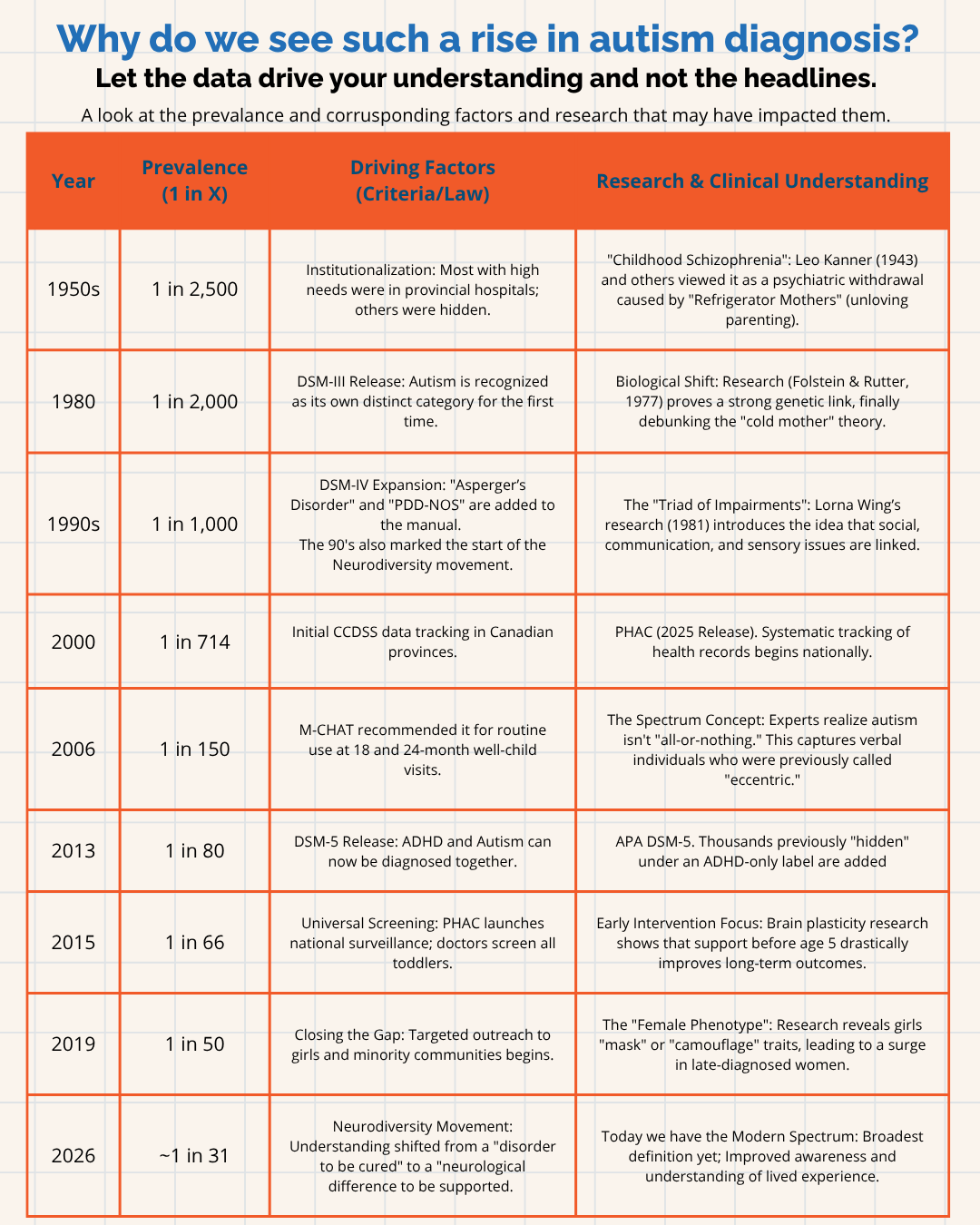
In the 1950s, the prevalence was estimated at just 1 in 2,500. At that time, based on work by Leo Kanner (1943), autism was viewed as a rare psychiatric "withdrawal." Many individuals with high support needs were institutionalized in facilities like Ontario’s Huronia Regional Centre, rendering them invisible to the general public.
2. The Biological Breakthrough (1977–1981)
The narrative changed when researchers like Folstein & Rutter (1977) proved through twin studies that autism was a heritable, biological brain difference—not a result of "Refrigerator Mother" parenting. Shortly after, the Camberwell Study (Wing & Gould, 1979) provided the foundational research that moved autism from a "rare disease" to a "common spectrum."
3. Opening the Gates (1994)
1994 was a watershed year. The release of the DSM-IV officially added Asperger’s Disorder and PDD-NOS. For the first time, individuals who were highly verbal and had average-to-high IQs were included in the count. We didn't "create" more autistic people; we simply stopped ignoring the ones who didn't fit the 1950s stereotype.
4. Universal Screening and the "Double Label" (2006–2013)
By 2006, the Canadian Paediatric Society moved from "waiting for parental concern" to universal screening (the M-CHAT). Then, in 2013, the DSM-5 allowed for a dual diagnosis of Autism and ADHD. Thousands of Canadians who were previously "hidden" under an ADHD-only label were finally accurately identified.
The "Uta Frith" Perspective: Is it an Epidemic or an Expansion?
The rise in diagnoses has naturally led to a debate about where the boundaries of autism should lie. Even pioneers in the field, such as Professor Dame Uta Frith, have recently suggested that the "spectrum" has expanded so far that the label is at risk of "collapsing"—becoming too broad to provide clear clinical direction.
From a traditional medical standpoint, there is a desire to return to a narrower definition that focuses primarily on "prototypical" autism—those with significant language delays or intellectual disabilities identified in early childhood.
After 40 years of supporting this community; when we look at how we understand autism over time, we have broadened the net to catch those who were going undiagnosed and unsupported. We are finally "closing the gap" for women, girls, and cultural minorities—groups that PHAC (2019) noted often "mask" their traits to survive in a neurotypical world. That is a good thing. However we categorize the individual aspects that make up autism we still need to help individuals build skills and advocate for systemic changes that make the world more inclusive.
At LRCSS, we view this not as a failure of the diagnosis, but as an evolution of our understanding. While earlier research (such as the "Theory of Mind" work in the 80s) provided a foundational understanding of autism, modern science has moved beyond observing only outward behaviors. We now understand:
The Reality of Masking: Newer research (such as Hull et al., 2020) has validated what many women and late-diagnosed adults have known for years: that "functioning" on the outside often comes at a massive internal cost of exhaustion and mental health strain.
A "Spiky" Profile: Autism isn't a linear scale from "mild" to "severe." An individual may have a PhD in astrophysics (low support needed in academics) but find it difficult to navigate a grocery store due to sensory overwhelm (high support needed in daily living).
The Diverse Spectrum: Instead of seeing the spectrum as "meaningless," we see it as a collection of diversity. As recent genetic and neurological studies (2025/2026) suggest, we aren't seeing "too much autism"; we are discovering "many autisms," each requiring its own specific, evidence-based approach.
Legitimate Concerns: There are legitimate concerns about how to fund and ensure support for individuals with complex needs while also addressing the growing needs of the newly diagnosed.
40 Years of Growth: Our Commitment to You
The "debate" over labels doesn't change the daily reality for the families we serve. Whether someone meets the "classic" criteria established 40 years ago or the broader criteria of today, their need for understanding and effective support is real.
At LRCSS, our mission and vision are rooted in the belief that everyone can thrive. Over our 40-year history, we have learned that:
Science is the Compass: We use evidence-based support to navigate the evolving landscape of neurodiversity.
Individualization is Key: Whether an individual has complex needs or is a late-diagnosed adult seeking social strategies, their support must be as unique as their fingerprint.
Respect for Identity: Whether you identify as autistic or your prefer person first language or you don’t focus on your diagnosis at all we respect how each and every client chooses to define themselves.
Knowledge is Power: When you know better, you do better. We are committed to constantly asking better questions and deepening our knowledge.
Just as society has changed, our definition/criteria of autism has changed. So we also adapt and will continue to do so to meet the needs of everyone we serve. As we celebrate our 40th anniversary, we remain dedicated to creating an inclusive society where everyone can thrive.
SOURCES:
1. Foundational & Historical Research
Kanner, L. (1943).Autistic Disturbances of Affective Contact. Nervous Child, 2, 217–250.
The origin of "Infantile Autism" as a rare psychiatric condition.
Folstein, S., & Rutter, M. (1977).Infantile Autism: A Genetic Study of 21 Twin Pairs. Nature, 267(5614), 792–794.
The first major study to prove autism is biological and heritable, debunking the "Refrigerator Mother" theory.
Wing, L., & Gould, J. (1979).Severe Impairments of Social Interaction and Associated Abnormalities in Children: Epidemiology and Classification. Journal of Autism and Developmental Disorders.
The "Camberwell Study" which first introduced the "Triad of Impairments" and the concept of a spectrum.
Wing, L. (1981).Asperger's Syndrome: A Clinical Account. Psychological Medicine, 11(1), 115–129.
The paper that introduced Asperger’s to the English-speaking world, expanding the diagnosis to verbal and high-IQ individuals.
2. Diagnostic Manuals (Evolution of Criteria)
American Psychiatric Association. (1994).Diagnostic and Statistical Manual of Mental Disorders (4th ed.). Washington, DC.
Formalized the inclusion of Asperger’s Disorder and PDD-NOS.
American Psychiatric Association. (2013).Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA.
Merged all subtypes into "Autism Spectrum Disorder" and removed the prohibition on diagnosing Autism and ADHD together.
3. Canadian National Data & Screening
Public Health Agency of Canada (PHAC). (2018/2019).Autism Spectrum Disorder Highlights: Canadian Health Survey on Children and Youth. * The data set that first established the "1 in 50" (2.0%) prevalence for Canadian youth.
Public Health Agency of Canada (PHAC). (2025/2026).Understanding Autism Data in the Canadian Chronic Disease Surveillance System (CCDSS). * The most recent release (Dec 2025) showing the rise from 1 in 714 (2000) to roughly 1 in 44 (2024-2026), with some regions like PEI reaching 1 in 34.
Canadian Paediatric Society (CPS). (2019/2024).Early Detection for Autism Spectrum Disorder in Young Children. * The clinical guidelines mandating routine screening (M-CHAT) in Canadian pediatric offices.
4. Modern Perspectives & "The Debate"
Hull, L., et al. (2020).Camouflaging in Autism: A Systematic Review. Social Science & Medicine.
Critical research on "masking," explaining why women and girls were historically underdiagnosed.
Frith, U. (2026).The Collapse of the Spectrum. (As cited in UCL News/The Telegraph, March 2026).
Uta Frith’s recent commentary arguing that the spectrum has become too inclusive to remain clinically predictive.
Livingston, L. A., & Happé, F. (2017).Conceptualising Compensation in Neurodevelopmental Disorders. Trends in Cognitive Sciences.
Research explaining how high-IQ individuals "compensate" for difficulties, often leading to late diagnosis.